


I've given a few presentations about Lean and mass vaccination clinics, based on my visits (as a guest observer / learner and as somebody being vaccinated).
Much of what I observed (and have shared) are good practices related to patient flow and preventing delays for patients.
That relates to the first pillar of the Toyota Production System — “Just in Time.”
There's also a second pillar that too often gets ignored — “Jidoka,” a word that can be translated to mean things like “quality at the source.” How do we build in quality? How do we ensure quality? How do we prevent errors?
Again, those are equally important concepts and they go hand in hand. Better flow (Just in Time) helps lead to better quality and better quality helps ensure flow is not interrupted.
I was originally going to release this blog post tomorrow morning, but I got a Moderna vaccine booster yesterday… and have been struggling through a high fever. Long story short, the pharmacy was misinformed and gave me a FULL 0.5 mL dose of vaccine, not the 0.25 mL dose.
Below is what I shared on LinkedIn. I'll write another blog post about all of the process problems I saw at CVS before and after getting the incorrect dose injected.
It has happened to others:
Back to the original post… as I posted about last week on LinkedIn, I heard a news story on NPR about the pediatric version of the Pfizer Covid vaccine:
FDA says the Pfizer COVID vaccine looks effective for young kids
The story mentioned, as an aside, a detail that seems very important to me:
“…in special orange-capped vials to distinguish them from adult vaccine…”
Below, you can see the adult dose (with the purple cap) and the pediatric does (with the orange caps and orange stripes on the vial label:

In terms of good process, vaccination workers probably shouldn't be popping the vial caps off before they are used. But, if somebody did do that (and I'll guarantee it happens somewhere), the vials still look different — the orange stripes indicating that it's a pediatric dose.
Now, some might say, “Well, people are ALWAYS supposed to read the label before drawing up a syringe.”
Yes, that's true, and the error proofing doesn't eliminate the need to read labels.
But, we're all human. We all make mistakes. We put the “human” in “human error.”
We can't just tell people to not make mistakes. We're not robots. We get fatigued. We get distracted. Our eyes (and our brain) sometimes play tricks on us — we think we are seeing something, but we're not.
The error proofing here, with the colors, might not be perfect. I don't think “orange / purple color blindness” is very prevalent (if that even exists). But, I'd rather see this attempt than none at all.
There are additional measures we could take, process wise, to make sure adult does and pediatric doses aren't ever co-mingled in a way that could allow them to be mixed up.
As an adult, I wouldn't want the smaller pediatric dose. And, we don't want children getting an inappropriately large dose either.
Other Errors — Same Color Caps
There was at least one case I read about where an error occurred, and similar packaging may very well have been a contributing factor or cause:
“Both the Moderna vaccine and the Regeneron monoclonal antibody are available in 5 mL glass vials. Vials of both the Regeneron antibodies and the Moderna vaccine have identical red caps.”
Patients were mistakenly given the antibody treatment instead of the vaccine, as explained here on the Institute for Safe Medicine Practices website. The composite photo below shows a vaccine, left, and two different Covid treatments, to the right.
Two different types of antibodies? And they both have red caps??
Yes, two different monoclonal antibody treatments have VERY similar looking vials, which can lead to confusion and error, as described here:
Handling monoclonal antibodies from Lilly and Regeneron can be confusing

Again, don't be tempted to say, “Well, if people would read the labels, there wouldn't be a problem.”
We're all human. When you're tired and under stress (as many healthcare workers are today), then errors are more likely to occur.
42 people in West Virginia mistakenly given Regeneron antibody treatment instead of the coronavirus vaccine
“It has been determined that this was an isolated incident,” Julie Miller, an administrator for the Boone County Health Department, told ABC News.
Being an “isolated incident” doesn't mean that it can't happen again. What change was made to the process? What actions were taken if we can't easily (or quickly) change the packaging that comes from the producers??
“While this injection is not harmful, it was substituted for the vaccine. But this occurrence provides our leadership team an important opportunity to review and improve the safety and process of vaccination for each West Virginian,” Dr. Clay Marsh, the state's COVID-19 czar, said.
Yes, every occurrence of error is an opportunity to improve. I believe we shouldn't blame or punish individuals for simple “human error” — it's counterproductive and it's unjust. If there wasn't INTENT, then don't blame or push — fix the system instead.
I'm paraphrasing Dr. Atul Gawande pretty closely when he said, of “checklists” as a form of error proofing, that good systems and good processes “help protect a great provider from having a very bad day” (as the result of making an error).
Heparin vs. Heplock
The issue of confusing look-alike medication packaging is not a new issue. Long-time regular readers of the blog will remember these posts:
Dennis Quaid And Medical Mistakes Episode On Oprah
The Quaid twins were harmed because they were given adult-dose heparin instead of hep-lock. See how similar the vials looked:
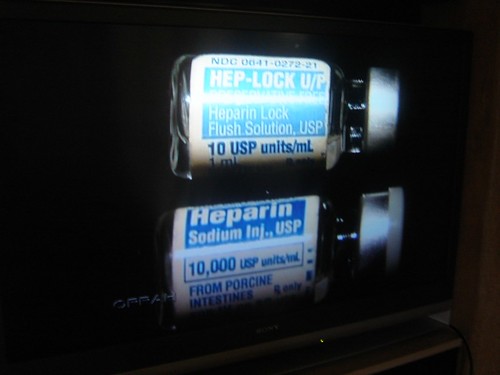
Not identical, but close enough. Especially at 2 am in a dark room with a fatigued provider.
A redesign of the packaging created both 1) a different look and 2) a different action required (breaking a paper seal or not):

And in a more light-hearted example that we might deal with in everyday life:
These Two Things Are Designed Badly, But Nobody Gets Hurt…
Spoiler alert, it's about coffee K-Cups:

What can we do to better error proof against these mishaps in vaccination?
- Giving the wrong vaccine as a second dose or booster
- Giving a full vial of the Pfizer vaccine instead of diluting it properly
- Giving an injection of 100% saline diluent instead of the vaccine mixture
- Giving a treatment instead of a vaccine (or vice versa)
- Giving a Covid vaccine instead of a flu vaccine
- Giving an adult dose to a child (or vice versa)
- NEW: Giving a full dose instead of a booster dose
These are all risks. These errors all happen — or are bound to happen — without great processes and without a culture of psychological safety. Without psychological safety, people don't speak up when they identify risks and they might be far less likely to speak up when an error does occur.
Too Many Errors
I shared just a few of the headlines about vaccine-related errors in the talks I have given…
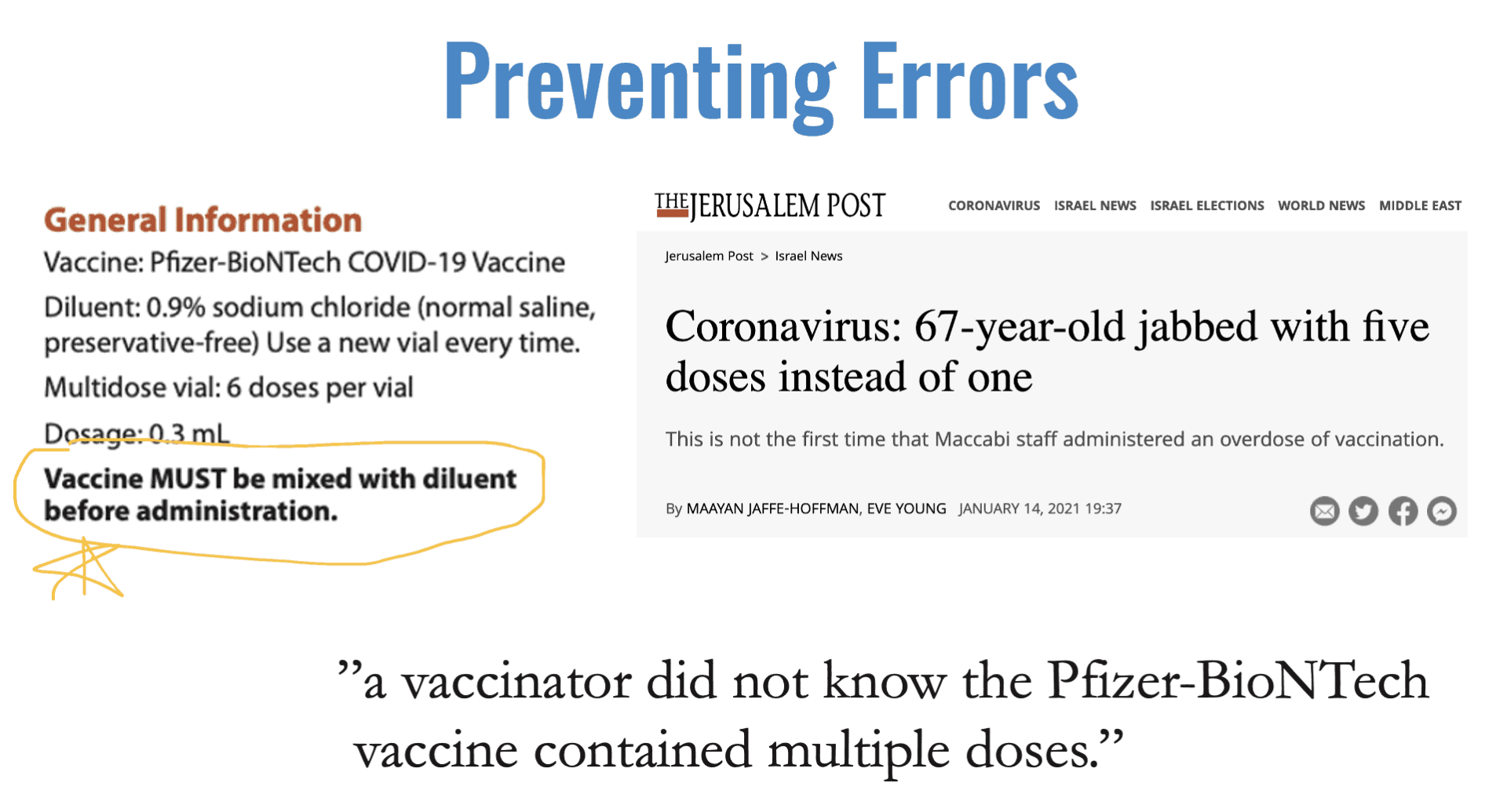
Coronavirus: 67-year-old jabbed with five doses instead of one
The CDC process instructions for giving the Pfizer vaccine clearly say you MUST dilute it.
But, how does a vaccination “not know” this? Who was managing that operation? Instead of blaming the vaccination, whose fault is it that the vaccination didn't get proper training and education? That's a systemic problem, not an individual problem.
Note the subheadline that says “not the first time” that the hospital staff in Israel made that same error. Systemic errors tend to be repeated by different people on different days if we don't fix the underlying system problems.
Another headline I've shared:
5 doses of Covid-19 vaccine given to S'pore National Eye Centre worker due to human error
From the article, we learn:
“…due to human error resulting from a lapse in communication among members of the vaccination team.”
Any time “human error” is blamed, we know it's really a process problem. Why was there a “lapse in communication” and why was that even possible?
“…the worker in charge of diluting the vaccine had been called away to attend to other matters before it was done. -A second staff member had then mistaken the undiluted dose in the vial to be ready for administering.” •
We've known for a long time that distraction is a huge contributor to medication errors. Why was that even possible? Why was the worker called away? Why was the status of said vials not 100% crystal clear? Again, those are systemic problems. It wouldn't be “just” to fire an individual here.
From Australia:
Elderly patients show no adverse reactions after being given incorrect dose of COVID-19 Pfizer vaccine
“The medical mishap has been blamed on a doctor who did not complete the mandatory online vaccine training prior to his first engagement…”
Are they blaming the doctor for not completing the training? Why not blame the group that didn't ensure that “mandatory” really meant mandatory? Why is anybody allowed near the vaccine without confirming that they not only completed the training… but understood it as well?
Wrong Vaccine For Second Dose Given at Suburban Chicago Mariano's
…our team is investigating the matter and will take steps to prevent a similar situation from recurring in the future.”
I hope they did take steps that were actually preventative in an effective way…
More and more errors:
Dozens potentially given harmless saline injection instead of COVID-19 Pfizer vaccine in Melbourne mix-up
The saline is “harmless.” Thinking you're actually vaccinated when you're not… that's harmful.
4-year-old child accidentally receives COVID-19 vaccine
If people are blaming “human error,” then what's the solution?
HINT: The solution is not removing humans from the equation… whether “removing” means automating them out of a job (not possible today) or punishing them for the error.
We need well-designed systems (as we discussed in yesterday's podcast) and we need the psychological safety that helps lead to continuous improvement as we attempt to perfect said systems. We can't just hang signs, re-train people, and tell them to “be more careful.”
Related Post:
Please scroll down (or click) to post a comment. Connect with me on LinkedIn.
Let’s build a culture of continuous improvement and psychological safety—together. If you're a leader aiming for lasting change (not just more projects), I help organizations:
- Engage people at all levels in sustainable improvement
- Shift from fear of mistakes to learning from them
- Apply Lean thinking in practical, people-centered ways
Interested in coaching or a keynote talk? Let’s talk.
Join me for a Lean Healthcare Accelerator Trip to Japan! Learn More







{kind=link}
I’ve been documenting more errors as comments on my post about my error, but here’s one where the mistake proofing was insufficient:
https://nypost.com/2021/11/12/virginia-pharmacy-gives-112-kids-wrong-doses-of-covid-vaccine/
Comments are closed.