


The theme for the next couple of days on the blog is patient safety and the idea of “psychological safety” for employees or physicians in the healthcare environment.
On Wednesday, I'll be releasing a podcast with Harvard Business School Professor Amy C. Edmondson, talking about her excellent book The Fearless Organization: Creating Psychological Safety in the Workplace for Learning, Innovation, and Growth.
Today, we'll explore what it's like to NOT have psychological safety in a hospital (or not enough safety). The other day, my friend Russell Watkins, from the UK, tweeted a photo of a newspaper story:
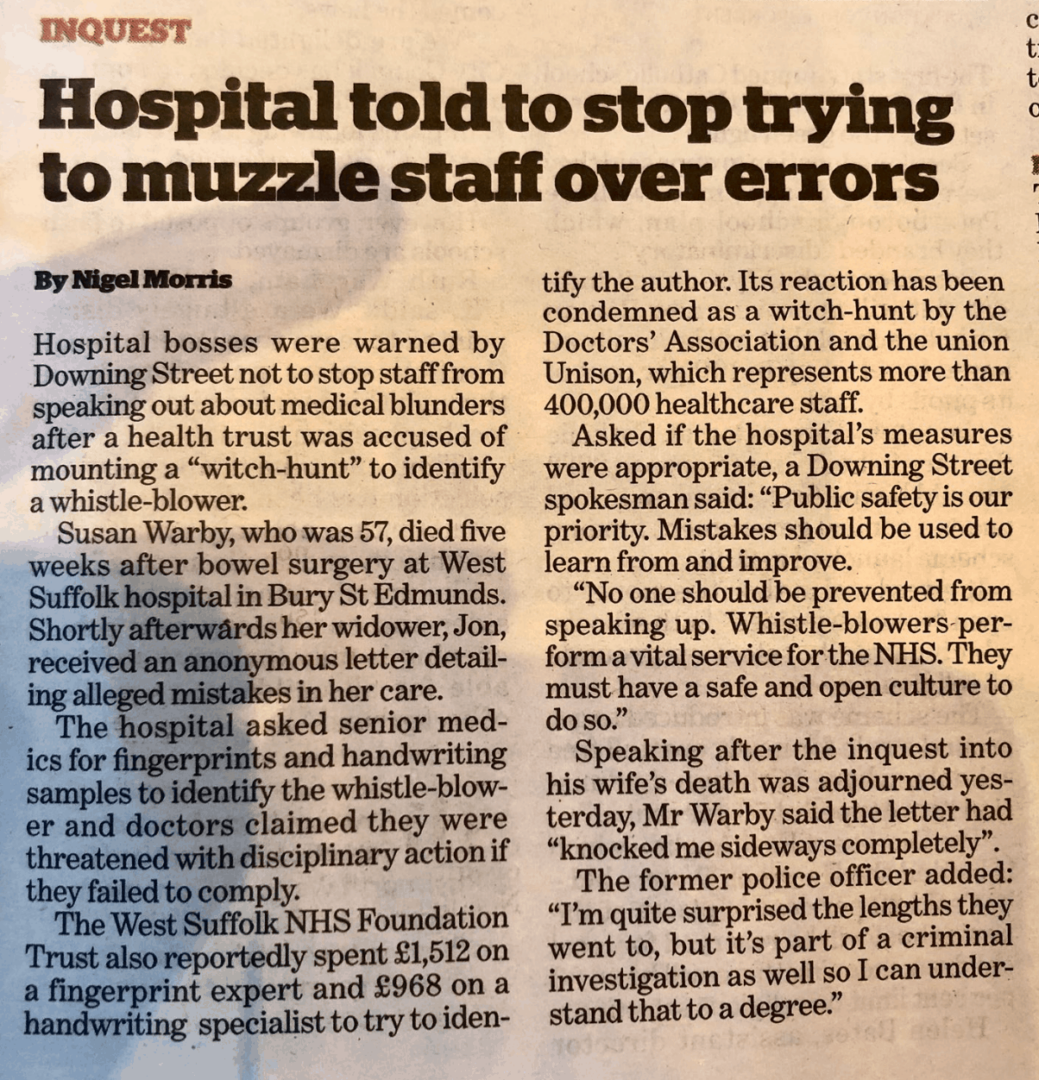
In summary, a patient died after surgery and her widower received “an anonymous letter detailing alleged mistakes in her care.”
The hospital when went on a “witch hunt” — trying to identify the whistleblower through fingerprints and handwriting analysis.
Talk about NOT getting to the root cause.
There's the question of “what are the root causes of the errors that led to the death?” There's also the question of “why are staff sending anonymous letters?”
I'm guessing that the writer of letter would LOVE to take care of this in a manner that's above board. It sounds like the hospital might have a culture of fear and intimidation. Maybe they have tried speaking up in the past (or they did speak up) and nothing constructive came of it.
I can't find that exact article online, but I found some recent history, including this article about the hospital in question, from December
Doctors at West Suffolk hospital ‘too scared' to report safety issues
“Staff are scared that they'll face disciplinary action [if they raise concerns about patient safety],” said one doctor, who declined to be named.
It's not surprising that the doctor is afraid to have their name associated with the idea of being afraid of speaking up. And, of course, I'm not blaming the doctor for being afraid. This problem starts with leadership.
On Wednesday, I'll ask Edmondson what she thinks about situations where I've heard people say things like, “Healthcare professionals have an obligation to speak up.” That's easier said than done.
The doctor added
“As a result of recent events I can't imagine that anyone at the trust will feel comfortable to speak out or whistleblow in the future. I fear that any future patient safety concerns will not be expressed and will simply be brushed under the carpet.”
See, when people aren't allowed to speak up about problems or risks, that hampers or prevents problem solving. Problems being “brushed under the carpet” means other patients could be harmed or killed by problems that aren't solved to root, in a way that prevents future occurrences.
Somebody else shares my suspicion that the whistle blower had no other outlet:
Another staff member said: “My colleagues in the hospital's surgical department have been hung out to dry over this [Warby's care]. Someone went to the family directly because they didn't feel the processes in the trust would investigate the safety issues effectively.”
The widower was surprised to hear about the “witch hunt.”
Widower ‘surprised' by hospital's fingerprint hunt for whistleblower
That article also details the error a bit:
The inquest heard that during one of Mrs Warby's operations the wrong fluid had been used in an IV drip. Instead of saline, a solution containing glucose was injected into Warby's artery and as a result her blood sugar increased to very high levels. Doctors did not realise the mistake and then treated her with insulin to bring the blood glucose levels down, despite the risk this carried of brain damage. The inquest also heard that Warby's lung had been punctured during a procedure to insert a central line into her inner jugular vein.
The hospital spokesperson seems to imply there's not really a culture problem:
A spokesperson for West Suffolk trust said: “We have a number of methods in place for staff to anonymously report patient safety concerns to the organisation, so that staff always have a way of speaking up, and our doctors routinely report concerns to us as is their professional duty.
“Any allegations that our staff have been bullied are taken extremely seriously and are investigated, which is one of the reasons why we are among the top five NHS trusts in the country for having engaged, happy, and empowered staff. We will continue to reflect as an organisation to address the concerns raised.”
That's all easier said than done. They might be empty words, just like a hospital spokesperson saying, after a medical error tragedy, “Patient safety is always our highest priority.” Is it? Is it really?
The second article I linked to includes these words from the widower:
He added: “The one positive to come out of all of this is the changes that have been put in place to protect future patients and prevent future incidents. Nobody should have to go through what we have been through.”
I hope they really have made changes — the right changes that will prevent future harm of this sort.
More from the news if you'd like to read additional stories about this case.
Even after being involved with healthcare for 15 years, I still get surprised (and saddened) when there is bullying, a lack of transparency, or other elements of organizational culture that hamper improvement.
A few years back, I was a consultant for a health system that had a broad Lean initiative. The CEO said he wanted the hospital to be the “safest in the state” by the year 2020. They had Lean activities, but there was a widespread and open fear of the CEO. People were definitely afraid of being fired for speaking up, disagreeing, or sharing data internally that didn't make everything look great.
I wondered (and never figured out) how a “culture of fear” was compatible with goals of being more safe. You can't flip a light switch and turn a culture of fear into a “culture of safety.” That CEO is no longer at the hospital and I'm guessing they can now make more progress toward that important aim.
Tomorrow, I'll share stories from Japan about two hospitals that ARE working to create a culture of safety in conjunction with their Lean / Toyota Production System efforts. I hope you'll come back to tread that post and then listen to the podcast with Edmondson on Wednesday.
Please scroll down (or click) to post a comment. Connect with me on LinkedIn.
Let’s build a culture of continuous improvement and psychological safety—together. If you're a leader aiming for lasting change (not just more projects), I help organizations:
- Engage people at all levels in sustainable improvement
- Shift from fear of mistakes to learning from them
- Apply Lean thinking in practical, people-centered ways
Interested in coaching or a keynote talk? Let’s talk.
Join me for a Lean Healthcare Accelerator Trip to Japan! Learn More







{kind=link}