


tl;dr summary: The blog post discusses the importance of reporting and solving problems for patient safety in Japan. It highlights stories from two hospitals that focus on patient safety and problem-solving, influenced by Toyota's methods. These hospitals strive for a culture of openness, where incidents are reported and addressed using problem-solving techniques, aiming for continuous improvement and psychological safety. The post emphasizes the need for a Just Culture and the adoption of TeamSTEPPS and Toyota's problem-solving steps to enhance patient safety.
As I blogged about yesterday, my theme this week is “psychological safety.”
Again, I'll mention that, on Wednesday, I'll be releasing a podcast with Harvard Business School Professor Amy C. Edmondson, talking about her excellent book The Fearless Organization: Creating Psychological Safety in the Workplace for Learning, Innovation, and Growth.
Here is that episode:
Yesterday, I blogged about a hospital in the UK that actively sought out a whistleblower who had reported errors to the widower of a patient who arguably died as the result of a medical error.
Today, I'd like to share some stories from visiting two hospitals in Japan this past December. Thanks again to Kaizen Institute for inviting me to partner with them in facilitating these study trips. Learn more about our next planned trip in June (and future trips).
A Focus on Patient Safety and Problem-Solving
Our group visited two academic medical centers in the Nagoya area. Both hospitals had a very strong (and admirable) focus on combining patient safety and problem-solving methods from Toyota.
The first hospital we visited talked about how they had “a very serious patient safety incident” back in 1999. They showed a photo of physicians and executives giving a deep bow at a news conference about the incident. This event “spurred a focus on patient safety.”
They also focused on changing the culture in ways that would lead to an increase in reported incidents and accidents.
Here is a chart that shows the increase:
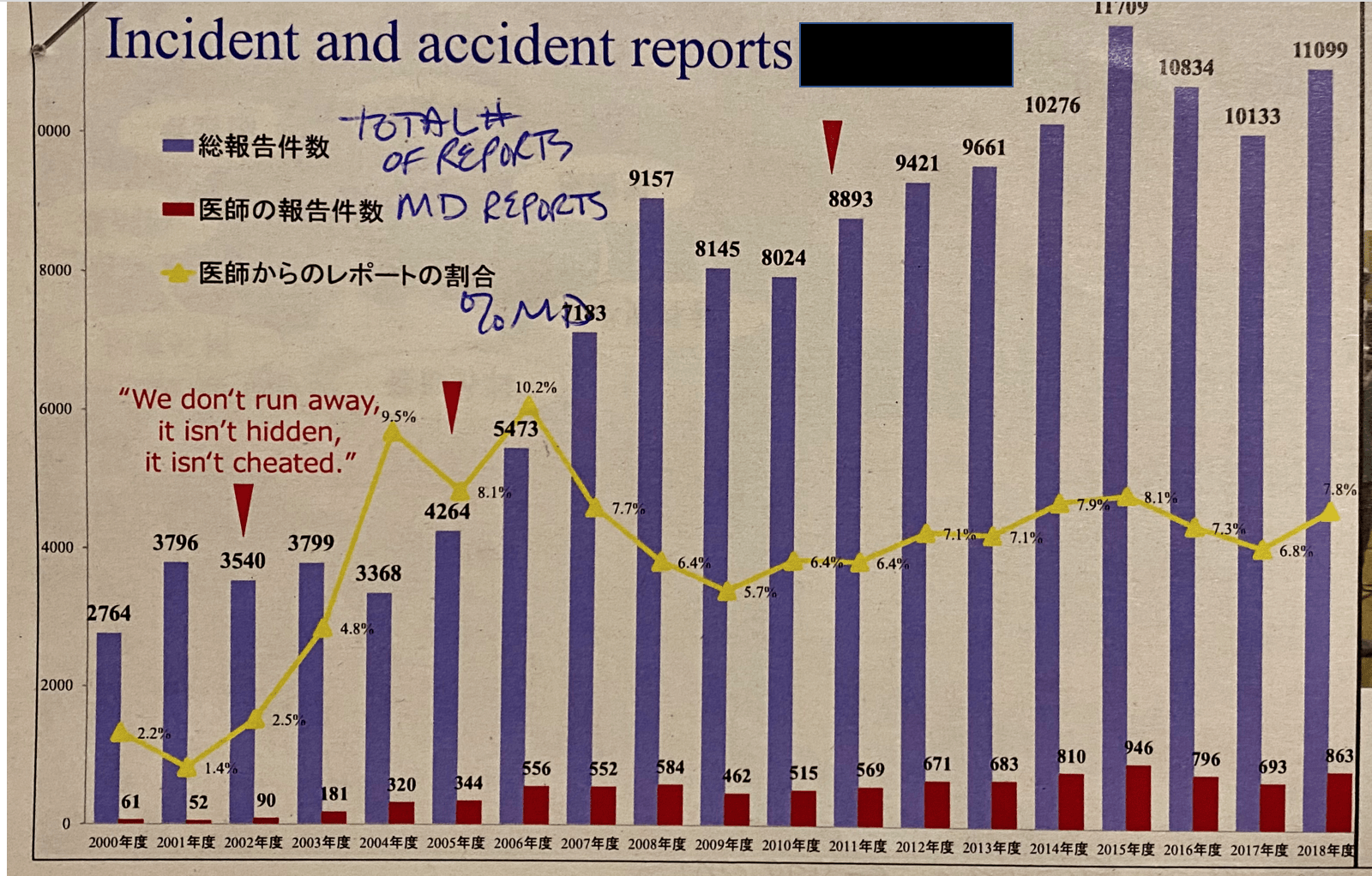
You'll notice that it says on the chart:
“We don't run away, it isn't hidden, it isn't cheated.”
The chart tracks the total number of reports, the number of reports made by physicians, and the percentage made by physicians.
The number of actual incidents and accidents wasn't going up. As they changed their organizational culture, the number of reported events caught up to the actual number.
You Can't Solve Problems If You Don't Identify and Share Them
At the second hospital academic medical center that we visited, they emphasized that if you don't identify problems (such as harm), you can't solve problems.
The second hospital was getting direct education and coaching on problem-solving from a high-ranking Toyota executive, a man who was the head of their Total Quality Management program. Yes, Toyota still uses that terminology. The second hospital emphasized, and I'm paraphrasing, that the Toyota problem-solving training would go to waste if they couldn't speak candidly about problems.
Speaking candidly about problems requires people to feel a sense of Psychological Safety. That's a universal human dynamic.
Here is their chart showing, again, reported incidents (which are similar numbers for these two similar-sized hospitals):
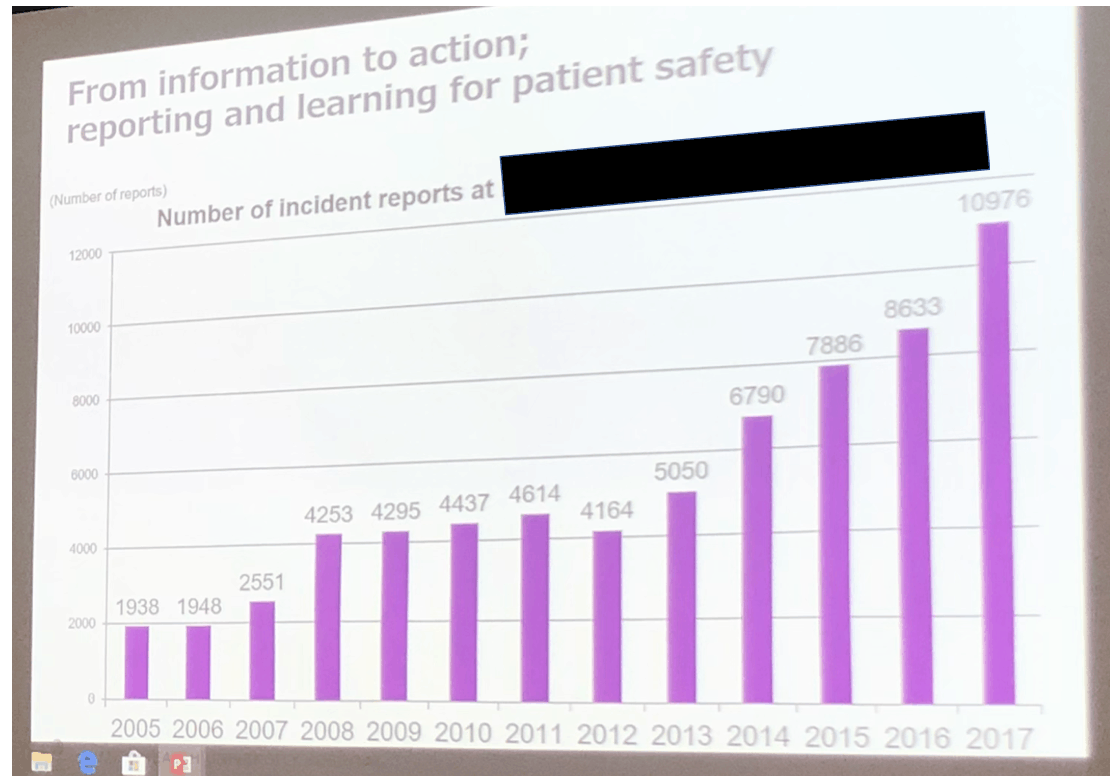
If leaders don't cultivate the conditions for Psychologically Safety, helping people feel safe to speak up, what chance is there for improvement?
I've seen data like this from other hospitals, including Virginia Mason Medical Center in Seattle. The number of reported incidents will go up for a while… and then that number hopefully goes down if the problem-solving is effective.
The first hospital said that many incidents were caused by “missing information” and it being:
“not safe to speak up.”
The hospital instituted a formal process for investigating medical accidents, with the goal of preventing recurrence — using PDCA cycles and a culture of learning.
Adopting Just Culture and TeamSTEPPS for Culture Change
The hospital also said they adopted the “Just Culture” philosophy and the TeamSTEPPS approach, which I love (and are very compatible with Lean).
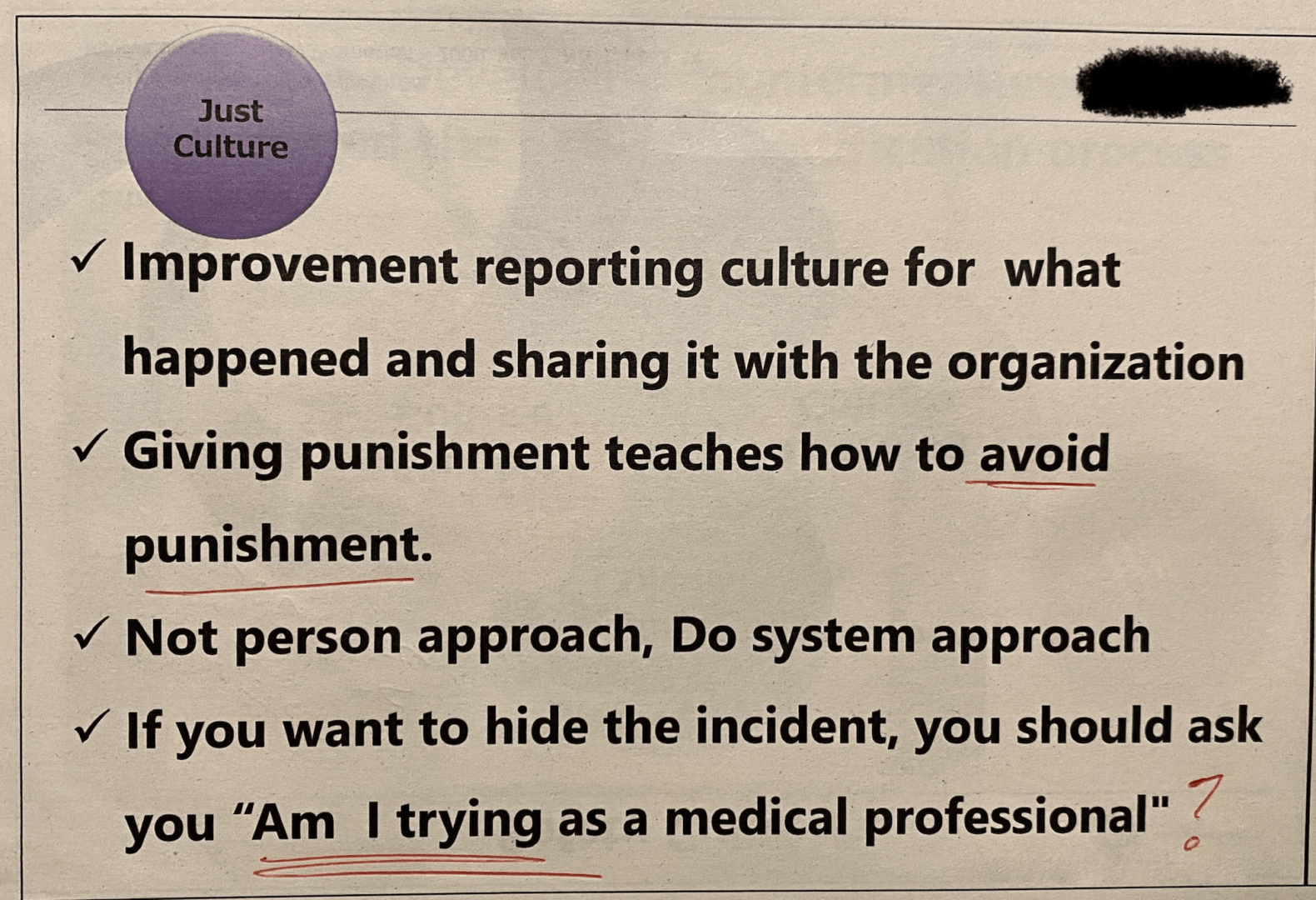
The slide above has a lot to unpack. They're working on the culture, focusing on systems instead of blaming people.
They further realize, thankfully, that blame and punishment can teach people how to avoid punishment, which often means hiding and covering up problems or pushing blame on others.
The last bullet point almost seems like they are trying to shame people into “doing the right thing” (although something could be lost in translation). I'm not sure that approach would work in all situations. If the culture is one where speaking up leads to blame and punishment, then the question of “Am I trying as a medical professional?” probably wouldn't help.
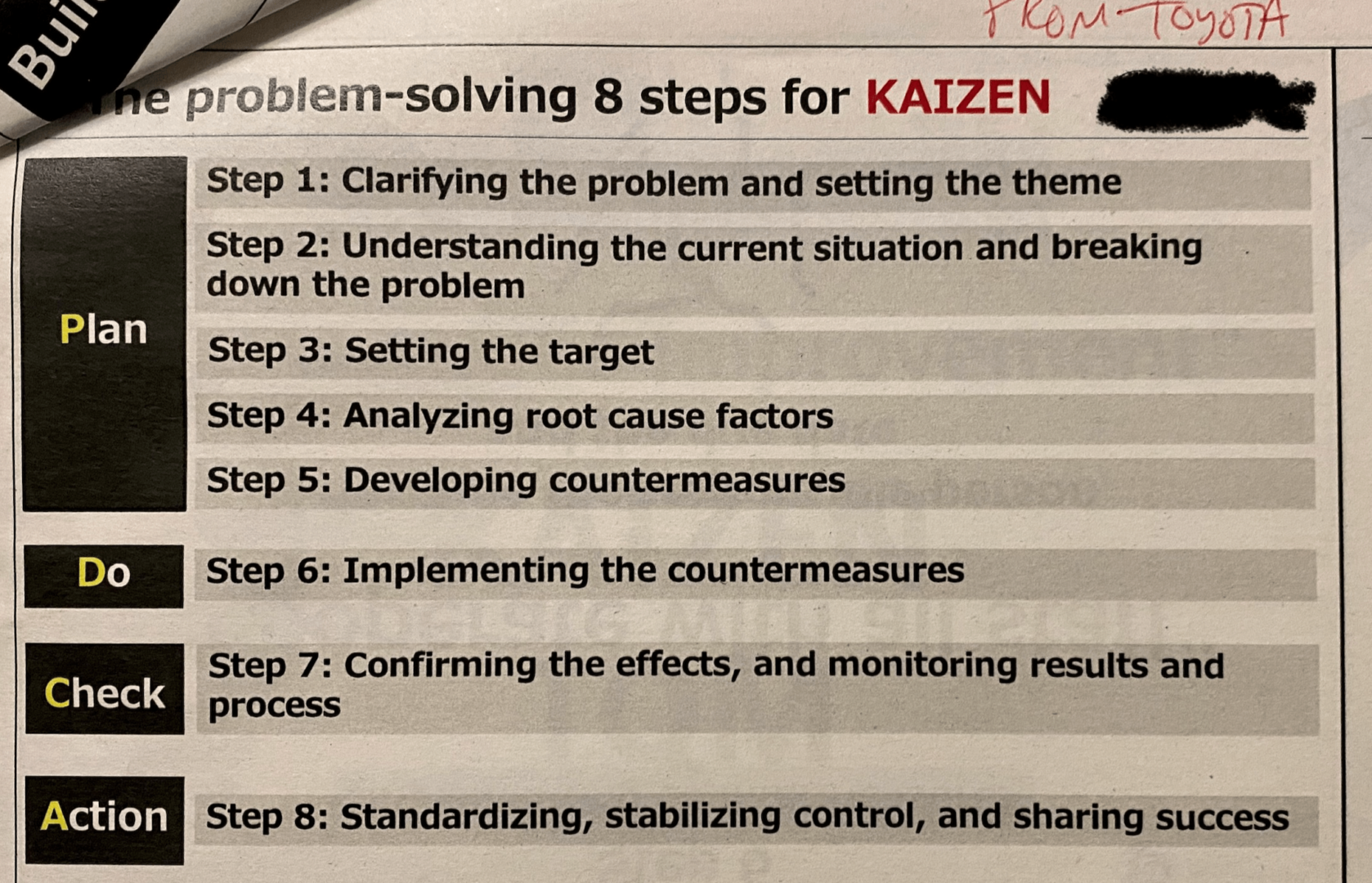
Learning Problem-Solving From Toyota:
The hospital leaders also said:
“Toyota taught us a lot.”
They “aim to use Toyota problem-solving steps,” as they illustrated below. This is basically a form of A3 problem-solving.
Another practice at the hospital is to focus on near misses. They said “most of” the incidents on the chart were “near misses,” not actual harm. We have to take advantage of the opportunity to learn from near misses, so we can prevent actual harm in the future.
The hospital talked about the “joy of Kaizen” but also lamented that “some MDs are not willing to commit to reducing harm” for various reasons.
They focus, though, on making safety a “daily operation, not one additional thing” to do.
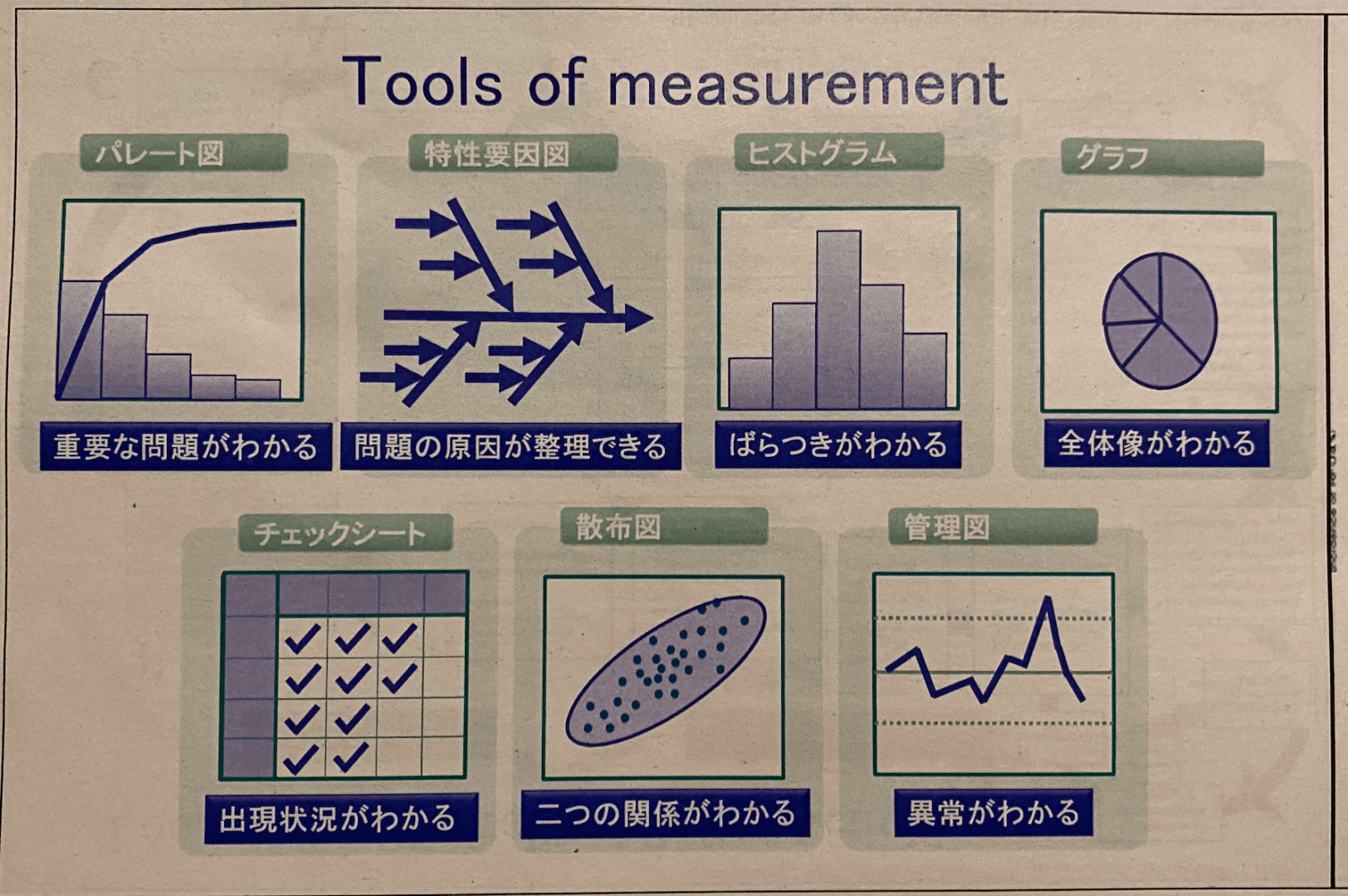
Diligently Using the 7 Basic Quality Improvement Tools
The hospital also uses what are often called the “7 basic Quality Improvement tools,” as illustrated below in Japanese. But, if you know these tools, the illustrations are enough to get the point across (the lower right is, of course, control charts).
The following thoughts stood out after Going through notes from the second hospital:
They aim to be “the safest hospital in Japan,” and the medical leader who is responsible for quality reached out to Toyota for help (their HQ is nearby). The Toyota leader, who we met the previous day, said he was initially skeptical that he could help a hospital. He said that the doctor “changed his life” through working together, and he hoped the doctor felt the same way (she did, as she said).
“Kaizen improvement will be a very strong engine for the hospital”
She said that Japan became aware of the need for improved patient safety around 1999 or 2000 (the same time as the U.S. “To Err is Human” report). There was an incident where the wrong surgery was performed on the wrong patient and another high-profile case involved an incorrect IV drip of a disinfectant solution being given to a patient — a fatal error.
Countermeasures and Influences
They have introduced many countermeasures in the past 15 years to help prevent errors, including:
- Sponges with x-ray contrast thread
- Also, counting before and after procedures
- Hand hygiene and standard precautions
- Reducing patient identification errors
They were doing many things, but one unintended consequence was increased burnout.
“As a result, the introduction of unpredictable redundancy exhausted medical staffs. We were not making staff happy, we were exhusting them.”
So, to find different ways of improving quality, they went overseas to teachers, including the IHI. They came to the U.S. to learn and people told them:
“You have a great teacher in Japan… Toyota.”
So, in 2010 she was inspired to learn from Toyota.
They were looking to shift the culture from one that was reaction-based to one where safety is just how we do things, “climbing the stairs.”
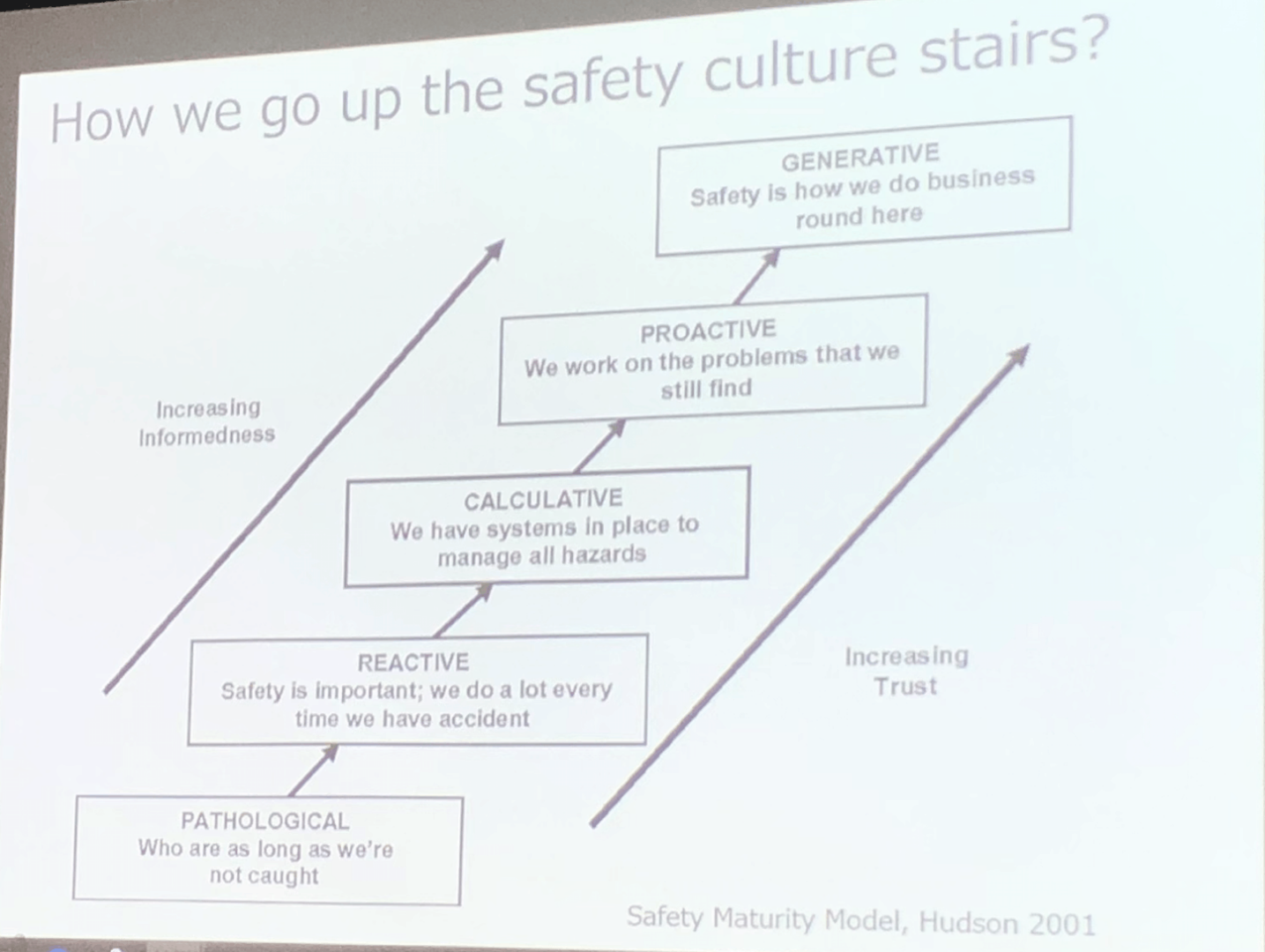
She said:
“An incident reporting system is required to move up from Reactive to Calculative. To go from Calculative to Proactive requires Kaizen”
She showed control charts of some key metrics, where the data points were not always in the “green” zone that is better than the goal.
She said:
“I prefer the red metrics because kaizen is my job. If it is perfect, there is nothing I can do.”
This hospital started by teaching A3 problem-solving to physicians. They've now evolved to working on engaging everybody in Kaizen — focused on patient safety and small Kaizens, as well. The hospital shared a larger A3-structured improvement effort that aimed to improve stroke care.
“Reducing stroke care time seemed impossible, but that became a catalyst for other improvement.”
Anyway, I think the two hospitals that I've written about today illustrated organizations that are working to increase the level of psychological safety in the organization.
Psychological safety means people feel safe to report incidents. This leads to increased incident reporting, which means more problem-solving (especially when you've been taught and coached by Toyota).
Please scroll down (or click) to post a comment. Connect with me on LinkedIn.
Let’s work together to build a culture of continuous improvement and psychological safety. If you're a leader looking to create lasting change—not just projects—I help organizations:
- Engage people at all levels in sustainable improvement
- Shift from fear of mistakes to learning from them
- Apply Lean thinking in practical, people-centered ways
Interested in coaching or a keynote talk? Let’s start a conversation.







{kind=link}
Hi Mark, I really enjoyed this post. I love the first hospital’s outlook which seems to be, culture eats strategy for breakfast which is so true! Your strategy will only work if your culture is aligned with it so when possible, it’s best to work on strategy first. The second hospital, second graphic “Just culture” reminds me of the book, The New One Minute Manager. Improvements or re-directs should be consistent and help to reach the end goal much faster!