


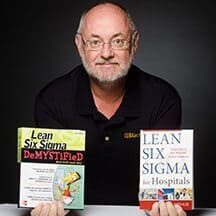
My guest for Episode #274 of the podcast is Jay Arthur, author of Lean Six Sigma for Hospitals: Improving Patient Safety, Patient Flow and the Bottom Line, Second Edition.
Jay is owner and founder of his company KnowWare International, based on Denver. Before founding that company in 1995, Jay was in a number of quality roles at US West / Qwest from 1973 to 1995. He has a BS in Systems Engineering from the University of Arizona.
Lean and Quality and Six Sigma
To me, “Lean Sigma” is often a controversial topic… not because anything is wrong with Six Sigma. Six Sigma methods can be very compatible with a Lean culture. But, “Lean Sigma” books and trainers (including Jay), paint a picture that says Lean is only about speed or efficiency and that Six Sigma is the method to improve quality.
He says pretty directly in his book that Lean helps fix all of the types of waste… except for the waste of defects. He says Six Sigma is used to address defects. That's silly.
The Podcast Discussion
I challenge Jay a bit about this in the podcast, and I'd like to remind the listeners that Lean and the Toyota Production System are about flow AND quality. Lean and quality go hand in hand. Lean methods, like error proofing, and mindsets, like not blaming people, can very directly improve quality.
So, I disagree with him on that point, but there are many good points in his book about not overcomplicating Lean or Six Sigma — that the goal is results (and I'd add “developing people”). I'm also glad that the phrase “Patient Safety” is in the subtitle of his book, as it is in mine.
You can read more about Jay and his bio here.
Streaming Player (Run Time 50:22)
If you want to listen to some of the debate about the role of Lean in improving quality, here is a short excerpt:

For a link to this episode, refer people to www.leanblog.org/274.
Topics and Links for this Episode:
- Jay's website
- Follow Jay on Twitter as @Knowwareman
- Find Jay on LinkedIn
- Please introduce yourself for the listeners… how did you get involved in process improvement and quality?
- When and how did you get involved in healthcare?
- What led to the writing of your book Lean Six Sigma for Hospitals?
- You make some good points in the book about not going overboard with Six Sigma… what are some examples of that? Why does that happen? What do you recommend?
- One thing I take issue with is the general Lean Sigma framework that says, “Lean is for speed and Six Sigma is for quality.” In your book you say “Lean will reduce wastes 1 through 6 and Six Sigma will help you to reduce number 7 (defects).” Why do you say or imply that Lean doesn't address defects when that's a core part of Lean and TPS?
- You say any “project” should generate a $50,000 savings… but what about cases involving quality and safety that are harder to quantify? Should every improvement be a “project?”
- How should Lean and Six Sigma be combined effectively in healthcare?
- What's new in the 2nd edition?
- Any last thoughts or advice for the listeners?
For earlier episodes of my podcast, visit the main Podcast page, which includes information on how to subscribe via RSS, through Android apps, or via Apple Podcasts. You can also subscribe and listen via Stitcher. Please leave us a review and rating!
Thanks for listening!
Podcast Summary
You can also read and download this 4-page PDF summary of the podcast:
Videos with Jay Arthur:
Please scroll down (or click) to post a comment. Connect with me on LinkedIn.
Let’s work together to build a culture of continuous improvement and psychological safety. If you're a leader looking to create lasting change—not just projects—I help organizations:
- Engage people at all levels in sustainable improvement
- Shift from fear of mistakes to learning from them
- Apply Lean thinking in practical, people-centered ways
Interested in coaching or a keynote talk? Let’s start a conversation.







{kind=link}
Some images and quotes you can share via social media:
The amount of tools you need in the healthcare environment is very small compared to what you might need if you wanted to go out and optimize a plant that makes carburetors”.
Wow. I’ve spent a lot of time in both manufacturing and healthcare, and I think this is fundamentally and demonstrably untrue. Trying to understand healthcare from HBR articles and Press Ganey surveys will give you a different perspective than actually immersing yourself in hospital process improvement. His ED throughput anecdote is a prime example. Many ED throughput success stories often leave out the true outcome of some of these projects (shifting waste to radiology/labs/inpatient, increased volume of antibiotic and opioid scripts, negative impact on rev cycle, etc). This is what happens when we try to fix “processes” without actually understanding the “system”.
SMED, MSA’s, FMEA’s, takt time, multi-vari analysis, etc are all traditional manufacturing tools that are used everyday to drive transformational improvement in hospitals. These aren’t just carburetor shop tools.
That’s Jay’s opinion, not necessarily mine.
I still cringe at the “tools” discussion. Lean is not just a set of tools. Lean is not “just another tool in the process improvement toolbox.”
I’ve noticed people who started with a Six Sigma background tend to say that more than people who started with Lean and then learned Six Sigma.
Personally, I learned statistics… then Lean/TPS… then more about statistics. I took a Green Belt class, but didn’t get certified.
Totally agree re tools. No organization ever went bankrupt because they didn’t know how to effectively implement a 2-bin kanban system or execute a really good DMAIC project. Companies struggle when they don’t establish a culture and system infrastructure that creates alignment and focus around the small number of things that they’re really trying to do as an enterprise. It’s easy to promote tools and projects and stat software. It’s much harder to truly partner with an organization (particularly a hospital network) to really understand their system and build a sustainable capability. I think that’s the “Lean” as you and I see it, rather than “Lean” as a toolbox as some others see it.
For Jay or anyone else who is interested in helping to transform healthcare, I’d recommend spending some time in hospitals to truly understand the system. We can improve “efficiency” while worsening financial performance. We can improve patient satisfaction while worsening clinical outcomes. Go beyond mastering traditional process improvement methodologies and learn more about HEDIS, HCAHPS, Meaningful Use, and PCMH. Understand how customer satisfaction is fundamentally different in healthcare than it is in financial services or manufacturing. Understand how wait time in healthcare is fundamentally different than it is in retail or insurance. Understand WHY the healthcare system in India is different than the healthcare system in the US (and which best practices are transferable and which are not).
You can’t learn that by sitting in a booth at IHI. You learn that by putting in the time/work and humbling yourself enough to realize that there are more things that we don’t know about the system than there are things we know.